Published On Jan 23, 2017
Dr. Ebraheim’s educational animated video illustrates the condition of Sciatica nerve pain and its diagnosis.
About 3 million people suffer from sciatica and the condition usually resolves itself within a few weeks to a few months.
A few patients may end by surgery.
This problem of sciatica can be self- diagnosed.
What is sciatica?
It is a pain radiating along the course of the sciatic nerve which runs from the lower back to the buttock, through the back of the thigh and into the lower leg and foot.
Sciatica pain usually affects one side of the body.
Sometimes this pain is called “lumbar radiculopathy” or “true sciatica”.
Sciatica is not a diagnosis; it is a symptom of an underlying condition.
Sciatica Pain:
Pain is worse when sitting because sitting will place tension on the nerve, stretch it, and make it irritated and painful.
The pain is a nerve pain, it is sharp, shooting pain like electric shock, running down the leg with burning, tingling, pins and needles, the pain could radiate to the leg and the foot, and there might be some numbness.
The sciatic nerve originates from 5 nerve roots: from L4, L5, S1, S2, and S3.
All the 5 nerve roots join together to form the sciatic nerve, then it branch out again in the thigh and the leg to give multiple muscular/ motor and sensory functions to specific areas and specific muscles in the leg and foot.
What is the cause of the sciatica?
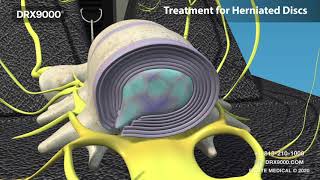
1- Lumbar disc herniation:
- A disc is a cushion between the vertebrae.
- These vertebrae have a soft inner material that may leak out or herniate from the disc through a tear in the outer fibrous layer, becoming a disc herniation.
- This irritates the close-by nerve root.
- Sciatica is one of the most common symptoms of lumbar disc herniation.
- MRI is the best study for diagnosing lumbar disc herniation.
- 90% of the patients will improve within about one month with nonoperative care such as: rest, physiotherapy, anti-inflammatory medication.
When do you do surgery?
When there is progressive weakness or persistent disabling pain for more than 6 weeks.
Who is a good candidate for surgery?
- A good surgery candidate will have: 1- sciatica (leg pain), 2- tension sign (positive straight leg raise), 3- abnormal neurological findings, 4- MRI finding which is consistent with the neurological examination.
What kind of surgery?
- Laminotomy.
- Discectomy.
- Surgery is better and is quick in recovery than no surgery.
- Surgery will cause improvement in the pain, in the function and satisfaction, however there is no significant difference in work status between surgery and no surgery at four years.
- After surgery, the patient can return to intense activity at 4-6 weeks.
2- Degenerative disc disease:
- Bony spur (osteophytes) may develop and press against the nerve.
- An L4-L5 disc involvement will affect the L5 nerve root.
3- Isthmic Spondylolisthesis.
- There are Pars defect, so the pars defect allows one vertebral body to slip forward on the other.
- Slip is a big deal, it is not a disc slipping, it is a slipping of the vertebral body.
- Slipping at the L5-S1 will involve the L5 nerve root.
- Slipping L4-L5 will compress the L4 nerve root.
- Slipping of the vertebral body cause the disc space to collapse and stress fracture, all will have the nerve to be pinched.
4- Lumbar Spinal Stenosis:
- Narrowing of the spinal canal and narrowing of the intervertebral foramen (nerve root canal).
- Hypertrophy of the facet joint, hypertrophy of the ligamentum flavum, disc degeneration, or arthritis are all examples of conditions which constrict the nerve root canals causing compression of the spinal nerves and sciatica.
- The patient will have back pain that is better with flexion, or leaning forward over a shopping cart.
- The pain will be worse with extension of the back.
- The patient will have leg pain, weakness, cramps, burning and heavy sensation.
- Neuroliogical examination is normal in over 50% of the patients and the straight leg raising is rarely positive.
- Differential diagnosis:
• hip disease or arthritis.
• Metastatic disease.
• Vascular problems.
- Every case that you suspect to be lumbar stenosis, suspect a
5- The Periformis Syndrome:
- The nerve could be irritated where it runs under the periformis muscle in the buttock.
- When the periformis muscle irritates the sciatic nerve, it causes sciatica.
6- Sacroiliac Joint Dysfunction:
- This doesn’t cause true radiculopathy, however the symptoms sometimes mimic radiculopathy or mimic periformis syndrome, and the clinician should be aware that these three entities can overlap and can mimic each other.